Obsessive-compulsive disorder (OCD) is a mental illness that causes intrusive, unwanted, disturbing thoughts (obsession). These obsessions are often followed by the urge to perform one or multiple actions in order to reduce anxiety and avoid the feared consequence (compulsion). The more the person engages in this circle of obsession and compulsion, the more salient and frequent the obsessions become, and the strongest the anxiety is, leading to a higher urge to perform compulsions.
This often results in the person spending large amounts of time performing compulsions (e.g., several hours checking), which interferes with work/school, relationships, and other aspects of day-to-day life.
There are different types of OCD, being the following some of the most common types:
- Contamination OCD: the obsession is the fear of being dirty or contaminated and the compulsion is, typically, cleaning and washing or avoiding places.
- Checking OCD: the obsession can be the fear of harm happening (e.g., a fire or a leak), and the compulsion is checking that everything is in order and okay.
- Symmetry and orderliness: the obsession is the idea that everything has to be in the “right way”, and the compulsion is ordering and organising things up until they are “just right”.
OCD is a serious condition and can be debilitating if not treated. Fortunately, there are scientifically proven successful treatments that can help people with OCD. Hence it is important to seek help if you recognise some symptoms that are affecting your life.
The main line of treatment for OCD includes therapy and medication (SSRIs). Specifically, the most effective therapy is cognitive-behavioural therapy (CBT) with exposure and response prevention (ERP).
In this page, we will explore further the mechanisms of the development and maintenance of the disorder, based on the CBT model of OCD, and how CBT and ERP work for this condition.
CBT model of OCD
Several theories explain OCD and its mechanisms, from behavioural to cognitive models. For simplicity, we will focus on contemporary cognitive-behavioural theories, as they best give a context for CBT with ERP treatment.
Although a number of cognitive-behavioural theories have been suggested, all share certain central principles and essential assumptions about the function of maladaptive thoughts in OCD. The figure below represents a general theoretical framework accepted by most of these cognitive-behavioural models.
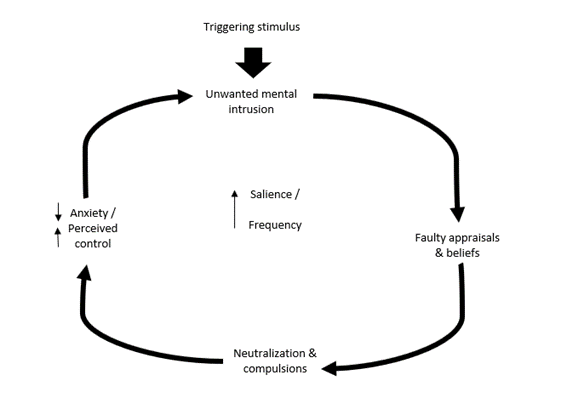
As seen in the figure, everything starts with a stimulus that triggers an unwanted mental intrusion, which can be a thought or an image. Nonetheless, it is not the intrusive thought in itself that leads to the development of OCD. In fact, it has been shown that intrusive thoughts are very normal in the general population. Numerous studies have uncovered that the majority of nonclinical people (80-90%) experience, at least occasionally, these types of thoughts that are comparable in content to the obsessions people with OCD have (Purdon & Clark, 1993; Freeston, et al., 1991; Clark, & Rhyno, 2005; Rachman & de Silva, 1978).
If intrusive thoughts are not what causes OCD, then what does? It is the faulty appraisals and beliefs, the way people that end up developing OCD interpret those thoughts that makes a difference. Those who don’t develop OCD let go of these intrusive thoughts quickly, they don’t give them any importance, regardless of how distressing and strange those may seem. People with OCD, however, get stuck in these thoughts and evaluate them as negative, they assign them meaning, they think they represent a real threat and that having these thoughts say something about their personalities (e.g., “I must be a bad person for thinking this”).
Researchers have classified the different types of evaluations a person with OCD tends to make, the most relevant being the following:
- Over importance of thoughts: consider that the simple presence of thought implies that it is relevant.
- Overestimation of threat: an exaggeration of the likelihood or severity of harm.
- Inflated responsibility: the belief that one has power that is crucial to bring about or prevent negative outcomes
- Importance of controlling thoughts: the overvaluation of the importance of exerting complete control over intrusive thoughts, and the conviction that this is feasible and desirable.
- Intolerance of uncertainty: ideas about the need of being certain, the belief that the person is unable to cope with unpredictable change.
- Perfectionism: the tendency to consider there is a perfect solution to every trouble, and that insignificant errors will have critical outcomes.
The different cognitive-behavioural theories agree that these faulty evaluations are necessary but not sufficient for reinforcing intrusive thoughts. A second step is needed to create an OCD circle difficult to break. This second step is the actions performed to control the thought, reduce the distress/anxiety or prevent the anticipated negative consequences related to the intrusive thought.
Together, faulty evaluations of the thoughts and the use of compulsions, neutralization or other control strategies are the two processes required to escalate an intrusive thought into an OCD obsession.
The result of the use of compulsions, neutralization, or other control strategies leads, in the short term, to the reduction of anxiety and an increased sense of control (as the anxiety reduces, also the sense of threat, which gives the false sense of control). However, engaging in these actions also increases the relevance and frequency of the obsessions. This is because, if the obsessions were not important, we would not need to do anything about them; however, by the mere act of doing something about it, we are telling the brain that that thought is important and we should be alert of any time we have that thought, so we can try to control it again.
The CBT treatment for OCD is based on this model and pays particular attention to both faulty appraisals and compulsions.
How does CBT work for OCD?
As in any other mental disorder, CBT therapy starts with an assessment, where the therapist gathers all the information needed to create a formulation of the problem and treatment plan. The therapist might ask about the different obsessions and compulsions, the frequency and intensity of those, etc.
The use of questionnaires is often helpful to gather as much information as possible, although some people may struggle to answer them due to their OCD. Always, the therapist would do their best to make the process easier for the person.
Once the therapist has the basic information, the work can begin. The treatment includes cognitive-behavioural therapy (CBT) with exposure response prevention (ERP), but different therapists differ on how they deliver these. Some prefer to focus on ERP first, while others argue that starting with CBT is desirable before starting ERP. In any case, the therapy is highly individualised, and the therapist will decide what is best for each person.
The CBT part of the treatment intends to reduce the faulty evaluations of the obsessions using cognitive techniques. The following components are typically included:
- Psychoeducation: learning how OCD works, the CBT model of the disorder, and the role of faulty evaluations/appraisals of the obsessions and compulsions/neutralization in the maintenance of the problem.
- Identifying and differentiating obsession and the evaluation of the obsessions: the obsessions and their appraisals become so habitual that can be difficult to differentiate. The therapist and client can work to recognise what is an obsession and what is the evaluation the person makes of that obsession (e.g., “this thought is important”, “the threat is high”).
- Cognitive restructuring tools: once recognised how the person evaluates the thoughts, tools to challenge these evaluations can be used. Remember that is those appraisals, together with the compulsions and control strategies that keep the OCD going.
- Alternative more helpful evaluations of the obsession: not only it is important to challenge the faulty evaluations, but it is also important to find alternative more realistic and helpful ways to evaluate the intrusive thoughts.
- Behavioural experiments: part of the work involves testing the faulty evaluations with experiments. Here you can read more about behavioural experiments.
- Relapse prevention: before terminating therapy, a review of the progress done is completed, as well as planning for possible lapses and setbacks.
These components are often combined with the ERP part of the treatment. Since the therapy is highly individualised, the therapist will work in a way that suits best the client.
Exposure and response prevention in OCD
Exposure and response prevention (ERP) is an essential component of the treatment for OCD. Through ERP the person exposes themselves to the feared situations and refrains to complete the compulsions or control strategies. This is done gradually, in a way that is challenging, but manageable for the person.
The first step in ERP is to create a hierarchy of situations the person is fearful of and sort it out by the level of anxiety each context would cause. Starting with a situation where the anxiety would be moderate, the aim is to face the fear and anxiety and challenge the faulty evaluations/appraisals by doing the things that trigger the obsession, without engaging in the compulsion.
For example, someone with contamination OCD could go to a public toilet (exposure) and refrain from washing their hands for 1 hour (response prevention – stop the compulsion). This exercise challenges several faulty evaluations and beliefs, such as:
- Overestimated threat: “I will get very sick from using a public toilet”.
- Inflated responsibility: “I will get contaminated from the toilet and spread it to others”.
- Intolerance of uncertainty: “I need to feel clean so I can be sure that I am not contaminated with any germ”.
After repetition and repetition of this type of exposure, the person gathers enough data to challenge these and incorrect other ideas. In the example, they can see that after going to a public toilet they don’t get sick and that even if they don’t wash their hands, the most likely outcome is that nobody around them gets sick either. Also, they discover that, although can be unpleasant, they can tolerate uncertainty and anxiety.
This part of the therapy can be quite challenging, but therapists are trained to encourage people and help them during this process, so it doesn’t have to be a lonely challenge. Engagement and commitment to the treatment are essential to get results, and it is worth it, as proven by many people that have overcome their OCD and improved their lives.
We can help with your OCD!
We understand how challenging and debilitating it is to have these obsessions and rituals and compulsions. Let us help you! We want to work with you. Contact us for any questions or bookings.